Danvers, MA, and Athens, OH
 Towering above the local landscape on a hill in northeastern Massachusetts are the remains of the Danvers State Hospital, its imposing clock tower still looming over the traffic on nearby I 95.
Towering above the local landscape on a hill in northeastern Massachusetts are the remains of the Danvers State Hospital, its imposing clock tower still looming over the traffic on nearby I 95.
Here, it is said, John Hathorne—one of the head judges of the Salem witch trials, known for his harsh interrogations, his presumption of the guilt of the accused—built his home. In the curious way that America sometimes piles one tragedy upon another, as if to quarantine the evil, the land that had been Hathorne’s became the site of the Danvers State Hospital, a place built with the best of all possible intentions that would, in time, be known as the worst of all possible worlds.
The hospital was made famous by H. P. Lovecraft, who used it as a model for his fictional Arkham Sanitarium. The real-life hospital was built in 1874 and has long had a host of legends attached to it. Even after the hospital was closed in 1992, its legacy as a haunted asylum remains.
If you call to mind a haunted mental asylum, you are undoubtedly thinking of Danvers: an ornate but sinister Victorian façade, long wings, and, in the center of the building, a glowering clock tower. This is no accident; Danvers is one of many asylums based on a similar model, a design by architect Thomas Kirkbride that was first implemented in 1848, at the New Jersey State Lunatic Asylum in Trenton. By the end of the nineteenth century, Kirkbrides dotted the country, from Salem, Massachusetts, to Salem, Oregon—home of the Oregon State Insane Asylum (where Ken Kesey’s novel One Flew Over the Cuckoo’s Nest was set). But within the past few decades, most of these buildings have been abandoned, demolished, or repurposed—few still operate as mental health institutions.
Danvers began shuttering its facilities in the late 1960s and shut down entirely in 1992. In 2006, after a lengthy process, a developer bought the property and set about renovating what was left of the asylum into luxury condos; the hospital’s massive wings were demolished, but the central administration building with its clock tower was preserved. Inside it smells of new carpet and fresh paint. If it feels eerie now, it’s perhaps not because of its provenance as a haunted asylum but because of its utter generic feeling: once you step inside its doors, you could be in any modest hotel chain in the country.
Unlike Moundsville and Eastern State, which were meant to exude a melancholy terror, their architecture part of the punishment, Danvers and its many sisters were designed to be welcoming, to reassure both patients and their families that they were in good, safe hands.
For centuries the mad belonged to the same group of society as the blind, the poor, the sick, and the elderly; all who could not work or otherwise easily contribute to society were more or less treated equally, regardless of the specificity of their situations. Prior to the rise of asylums, the mad were often sequestered in off-limits parts of their house. (Most famously, of course, in Jane Eyre, when Jane confronts the “madwoman in the attic,” Bertha.) But gradually, in the seventeenth and eighteenth centuries, the first madhouses began offering a place where wealthy families could sequester relatives. The madhouse, in this light, was simply the attic, or the basement, of the house, made external and moved elsewhere.
Early madhouses were often revealed to be nightmares of abuse and neglect. Reports of incontinent patients hosed down with icy water, naked women chained haphazardly to the walls, fleas and rats rampant, and other horrors gradually prompted a desire for something more sanitary and humane. In England, Bethlehem Royal Hospital—more often known as Bedlam—became so associated with chaos, horror, and depravity that its name has entered the dictionary as a catchall for chaos and lunacy.

In 1843 Dorothea Dix emerged as a powerful voice calling for social reform. In a memorandum sent to the legislators of her home state of Massachusetts, she railed against “the present state of insane persons confined within this Commonwealth, in cages, closets, stalls, pens! Chained, naked, beaten with rods, and lashed into obedience!” She found instances of inmates padlocked in cellars, left in the dark to wail in torment for years without aid or treatment. Something had to give.
The “moral treatment,” as it came to be known, became the solution: rather than chained and forgotten, patients would be unshackled and allowed to move about the asylum at will. Instead of being tortured and imprisoned, patients would work and play. Through labor and sports, hobbies and other recreations, the moral treatment promised rehabilitation and freedom from insanity. The moral model was held out as a means of actually curing patients, rather than simply bundling them out of sight. “All experience,” Dix claimed, “showed that insanity reasonably treated is as curable as a cold or a fever.”
The Kirkbride asylum came to be the architectural style most thoroughly associated in the United States with the moral treatment. Rather than terrifying, the new asylum would be inviting, surrounded by lawns and gardens that patients could tend themselves. The defining features of the Kirkbride asylum include the central administration building, stately and elegant, with a central tower and elongated wings, forming a shallow V that extends back farther and farther. Part of the beauty of this architectural model was that wings could always be added farther out indefinitely. As a result, they were often massive, growing to hundreds of thousands of square feet.
There was another reason for the ostentation in the Kirkbride design: while insanity, in its various forms, has accompanied humankind forever, the discipline of psychiatry was still nascent, and the idea of “treating” mental patients was not yet fully accepted. Kirkbride believed that, unlike other diseases, mental illness could not be treated at home, and required an institutional setting, but at the same time treated their asylums as home: doctors referred to themselves as “fathers,” the asylum as “the house,” the patients as “the family.” The asylum provided a large and visible monument to psychiatry. Built with sturdy stone, designed with grace and care, it made real the role of the psychiatrist; like a badge or a uniform, the building itself established authority and legitimized the discipline. People could see and point to it as a place of healing; it allowed people to see insanity as a disease that could be cured, and a psychiatrist as the doctor to cure it. It also became a clearinghouse for all the various maladies that could now be grouped under the notion of mental health. The asylum, in its own way, created both the doctor and the patient.
Dozens of Kirkbride asylums were built throughout the country during the second half of the nineteenth century. They became a way for middle- and upper-class families to transfer care of sick relatives to private facilities where professionals could assume the burden of care. They were inseparable from the burgeoning industrialization of the day; academic Benjamin Reiss refers to the asylum as a “laboratory for the purification of culture and the production of useful citizens.”
The Kirkbride asylum was meant to be the antidote to the kinds of horrific treatments at places like Bedlam. Why are we so afraid of them today?
Kirkbride asylums are, by design, huge. Danvers was originally 70,000 square feet, but this is modest compared with some of her sisters. The Trans-Allegheny Lunatic Asylum of West Virginia was 242,000 square feet; the Northern Michigan Asylum in Traverse City was, when completed, more than 380,000 square feet; Greystone in New Jersey and the Ridges in Athens, Ohio, were both more than 660,000 square feet.
Originally the asylums’ size and amenities were subsidized by the affluent families who wanted the best for their relatives. But in the wake of the Civil War, veterans began to crowd the only federal Kirkbride asylum in Washington, DC (the Government Hospital for the Insane, since renamed St. Elizabeths Hospital), and it became clear that insanity was not simply a problem for those with money.
By the second half of the nineteenth century, psychiatric care fell more and more under state control. Private Kirkbride asylums were turned over to the states, and many states built their own in imitation of the same model. For the first time size and cost began to be an issue.

Public officials balked at lavishing taxpayer resources on so few inmates. One opponent, Hervey B. Wilbur, tallied up the cost of various asylums alongside their relative capacities: Danvers, built at a cost of $1.6 million, was designed to house only 450 patients; the Ridges, built for $950,000 for just 600 beds; Worcester State Hospital in Massachusetts, built for $1.25 million for only 450 beds; Greystone, built at a cost of $2.5 million for just 800 beds; and so on. Wilbur ultimately estimated that the Kirkbride asylums were costing around $2,600 per bed—and that excluded the site’s land value and its furniture, to say nothing of its staff and upkeep.
The solution seemed to be to take these great buildings and cram into them as many humans as possible. Buildings that were meant to be expansive and give patients a great amount of freedom were now stuffed with bodies, creating a downward spiral of deplorable conditions, under-staffing, overtaxed resources, and inhumane treatment.
Whatever the Kirkbride model promised by way of rehabilitation rates was effectively destroyed by this civic disengagement. The asylums became host to the worst kind of neglect and abuse that had typified their precursors—precisely what they had been designed to address.
By the end of the nineteenth century, the Kirkbride plan was being abandoned in favor of another form of architecture: the so-called cottage plan, which focused on campuses of smaller, freestanding buildings instead of giant, imposing façades. The Kirkbrides seemed anachronistic, reflective of an earlier age in which tax money was wasted on frivolous architectural details and massive floorplans.
In a short time the Kirkbride ideal went from being seen as progressive to being a symbol of neglect. And so the clock tower of the administration building became menacing and the loving touches meant to look like home became grotesque parodies.
Through it all the stately façade of the Kirkbride asylums remained stately, even if now the boastful architecture projected not sanity and sanitary conditions but a living nightmare. Stories of deaths inside the walls, bodies forgotten, “treatment” that resembled sadistic torture, gradually gave way to stories of ghosts, poisoned land, and haunted buildings.
The ghost stories surrounding the haunting of Kirkbride asylums, like the Danvers Hospital, often originate in a very real, very troubled past. Danvers quickly became notorious for its overcrowding, with almost four times as many patients as the hospital was designed to house. Patients sometimes died out of sight of the staff and their bodies decomposed for days before they were noticed. A report from 1939 noted that more than 10 percent of the asylum’s population had died within its walls. Add to the hospital’s grisly reputation the ignoble distinction of being the place where the prefrontal lobotomy was refined and widely implemented. It’s precisely this accumulation of horrors behind its walls that has led to the prevalence of spirits at Danvers and made it a mecca for paranormal enthusiasts. Thrill seekers trying to get access to the hospital even after it closed its doors led to heightened security on the property; more than 120 would-be ghost hunters have been arrested for trespassing since 2000.
Among those who claim to have seen things there is Jeralyn Levasseur, who grew up on the grounds (her father, Gerald Richards, was a hospital administrator). Levasseur recalls apparitions angrily scowling at her and her sister when she was a child, and once in high school her bedcovers were yanked off in the middle of the night without warning. Levasseur explained her experiences as a function of the changing nature of psychiatric health: “If you think back to the beginnings of medical science and the things done to people,” she told a local newspaper in 2003, “not because they thought they were doing bad, but because they were trying to do right, you have to wonder, did people think they were being tortured?”
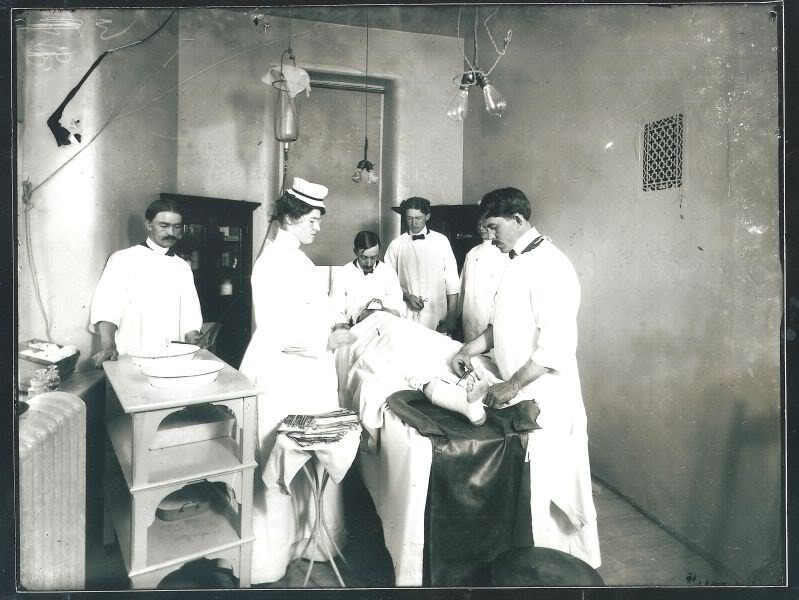
The history of the asylum, as with the hospital, is the history of practices that once seemed necessary and now strike us as bizarre and troubling. Dr. Henry Cotton, who from 1907 to 1930 was the superintendent at the Trenton State Hospital (the former New Jersey State Lunatic Asylum, first of the Kirkbrides), performed savage surgeries on his patients for decades, extracting everything from teeth to stomachs in the belief that infections were contributing to his patients’ psychological instability.
Haunted by such legacies, the ruins of the Kirkbride asylums—and their attendant lore—reveal how uncomfortable we’ve become with antiquated methods of “healing the sick.” Whatever the intentions behind them, lobotomies, straitjackets, and aggressive shock therapy now strike us as barbaric and unnecessary and hover in the back of our collective consciousness. As a culture we still struggle with unresolvable questions that were once wrongly answered in places like these: Who is crazy? Are we crazy? And what can we do to assure ourselves that we aren’t?
The stories of ghosts in the asylums are mostly driven by this anxiety, and for the most part they are the standard, vague stories without much substantiation. But if there is a particularly haunting symbol of the fall of the Kirkbrides—one that is verifiably real—it can be found in Athens, Ohio, in what’s left of the Ridges.
The Ridges first opened in 1868 as the Athens Lunatic Asylum—a monstrous campus stretching more than eight hundred feet long. Rather than the single central tower of Danvers, the Ridges is marked by the dual towers of the main administration building, giving its profile vague echoes of Notre Dame.
The plan included not just decorative lakes and fields meant to soothe wandering intellects but also gardens, orchards, and eventually a dairy barn, all tended by the inmates, in an effort to make the facility entirely self-sufficient. For a time it even played host to an alligator, which lived in its fountain during the summer months.
The asylum was built to house just over five hundred patients, but the population quickly grew to double that; like other Kirkbrides, the site soon faced overcrowding. By the 1970s it was underfunded and ill managed, with inmates poorly accounted for and large portions of the complex boarded up or otherwise not in use. In such a setting emerged a ghost story so compelling it ended up in the Journal of Forensic Sciences—that of the ghost of Margaret Schilling.
A patient of the Ridges’ Continued Care Unit, Schilling, then fifty-three years old, had general freedom of movement and no serious behavioral problems—she was a model patient, her behavior unremarkable in every way. But on December 1, 1978, she failed to show up for dinner, having disappeared without any sign. Within a few hours an extensive search was launched, with staff crisscrossing the wards in search of her. They didn’t find her that night—a worrying sign, given the brutally cold winter that had set in.
It wasn’t until January 11, 1979, more than a month later, that workers found Schilling’s body in the attic of an abandoned wing. There was no sign of foul play. Schilling appeared to have taken off her clothes and folded them neatly before lying down to die on the cold floor. No one could say how long she’d been dead, but despite the cold winter, the room had been warm enough to allow for significant decay.
She left behind no clues as to how she’d ended up there or what had led to her death, but she did leave behind a gruesome mystery: when workers removed her decomposing corpse from the concrete floor, they found a stain in the shape of Schilling’s body: a ghostly outline in chalky white, ringed by a fainter, darker outline. And despite how hard workers tried to clean the floor, the stain would not come off.
The stain of Margaret Schilling still remains. Over the years it’s been the source of numerous ghost tales and rumors about the hospital, but Schilling’s manifestation is not paranormal. A forensic team that investigated the stain in 2007 determined that the image was likely a result of a process called adipocere: the breakdown during decomposition of the body’s fat into soap. The investigators found a waxy residue on the floor that had significantly altered the chemistry of the concrete itself, leaving it lighter than the surrounding area. While usually adipocere requires moist, enclosed conditions (say, those of a coffin buried in the right kind of soil), the forensic team’s best guess was that Schilling’s corpse had undergone some similar process despite the less-than-ideal conditions of the attic.
This strikes me as far more terrifying than an actual ghost. That this woman, placed in the asylum’s care, was left to rot on this floor, her body imprinting itself on the cold, unforgiving concrete, seems more disturbing than any tale of an apparition or unidentified noise. Herself unable to tell her tale, Margaret Schilling nonetheless managed to leave an indictment of her caretakers, a savage rebuke of the years of psychiatry that has left a deep stain on our history.
 This regime of horrors wasn’t always evident. Family members and officials who came to tour these asylums often failed to see anything amiss. One of the benefits of the Kirkbride layout, with its gently flanking wings moving farther and farther away from the main administration building, was that it allowed the facility to segregate patients based on the severity of their condition. Traditionally the more difficult patients—the violent, the noisy, the untreatable—were housed in the wings farthest out, while the more sedate and promising patients were kept closer to the main building. Visiting relatives, shown the main building and the adjacent wings, left convinced that their relatives were in a stately, dignified place, not a madhouse. This was important, after all, so long as these institutions were private and depended on paying customers in the form of satisfied families. What went on behind closed doors would always remain a mystery.
This regime of horrors wasn’t always evident. Family members and officials who came to tour these asylums often failed to see anything amiss. One of the benefits of the Kirkbride layout, with its gently flanking wings moving farther and farther away from the main administration building, was that it allowed the facility to segregate patients based on the severity of their condition. Traditionally the more difficult patients—the violent, the noisy, the untreatable—were housed in the wings farthest out, while the more sedate and promising patients were kept closer to the main building. Visiting relatives, shown the main building and the adjacent wings, left convinced that their relatives were in a stately, dignified place, not a madhouse. This was important, after all, so long as these institutions were private and depended on paying customers in the form of satisfied families. What went on behind closed doors would always remain a mystery.
Stories began to emerge via the reports of those who’d escaped of horrors inside. Some of the more sensational of these came from a man named Ebenezer Haskell. Haskell was involuntarily committed to the Pennsylvania Hospital for the Insane in 1866 and escaped twice, the second time breaking his leg in the process. After a jury deemed him sane, Haskell wrote a book about his incarceration and trial in which he cited a number of horrific examples of patient mistreatment, including what he claimed was called the “Spread Eagle Cure,” a treatment that bore eerie similarities to the torture young Armstead Mason Newman endured in Lumpkin’s Jail:
A disorderly patient is stripped naked and thrown on his back, four men take hold of the limbs and stretch them out at right angles, then the doctor or some one of the attendants stands up on a chair or table and pours a number of buckets full of cold water on his face until life is nearly extinct, then the patient is removed to his dungeon cured of all diseases; the shock is so great it frequently produces death.
It’s hard to say for sure how accurate Haskell’s report was, particularly given his obvious axe to grind. But the lack of any clear information of what was going on, mixed with rumors and horror stories, only added to the picture the public began to form about the state of psychiatric care in general and at the asylum in particular.
The asylum in the nineteenth century embodies a tension between the visible and invisible—that is its most disturbing aspect. There is the highly visible and pronounced architecture, which projects one story, and there are the mostly invisible rooms on the edges, in the wings farthest out, hidden from public view.
Poe tapped into this tension in his short story “The System of Doctor Tarr and Professor Fether.” A visitor to an unidentified asylum in France (“a fantastic chateau, much dilapidated, and indeed scarcely tenantable through age and neglect,” one whose façade inspires the narrator with “absolute dread”) is shown a model of humane treatment, though gradually it becomes apparent that something is off. Only in the climax of the story is it revealed that the patients have overtaken the asylum; they’ve taken to impersonating the doctors, while the doctors themselves, along with the staff, have been locked up as patients. In the story’s final pages the doctors escape and riot; having been tarred and feathered, they unleash a terrifying fury on their captors, “fighting, stamping, scratching, and howling,” having been rendered less than human by their captivity. It’s a scene that speaks to the fine line between sanity and insanity. Once the doctors escape, they are as dangerous and as frightening as we’ve suspected the patients to be. Which is to say, once you’re inside the walls of the asylum, objective sanity is all but impossible.
Asylums became haunted by what happened inside their walls and also by the walls themselves: an architecture that was purposely boastful but which spoke of a previous generation with different ideals, economic motives, and attitudes toward the sick. The moment when we were most optimistic about our ability to cure the mind is when we built our most ostentatious palaces to psychiatry. There is a danger, then, in telegraphing too prominently one’s utopian ideals via architecture.
We design buildings not only for their utilitarian values but to project specific ideals and reflect our shared values. But these ideals and values are prone to change faster than the buildings. Shifting political fortunes, vacillating periods of excess and austerity, evolving attitudes about how the government should best serve its population—these all tend to move much faster than the time it takes for a building to outlive its usefulness.
“These are America’s castles,” Robert Kirkbride told me, speaking of the hospitals built on the plan of his ancestor Thomas Kirkbride. An architect and architectural historian himself, Robert was involved with the effort to save one building in particular: Greystone Park Psychiatric Hospital, in Morristown, New Jersey. Less than a year after it was closed, in 2008, a scheme to demolish the massive building and replace it with town houses was put forward by the city, only to be defeated by concerned citizens who argued that the hospital deserved saving: even as a gargantuan gothic ruin, Greystone was an important part of New Jersey’s history as well as a significant architectural landmark.
Cities have struggled to deal with these albatrosses—massive, unloved, associated with ghosts and an age gone by—as they’ve been decommissioned and treatment has moved elsewhere. Not only do they haunt our dreams; they haunt our local governments, who must figure out what to do with them. Many are on highly prized land that has developers salivating; even those that aren’t are massive buildings that require resources to keep them from falling into disrepair. They are filled with asbestos and lead paint—toxic materials that are another kind of civic ghost, a remnant of a former idea now discarded.
Danvers’s Kirkbride is a typical compromise, in which the most striking feature—the administration building’s façade—was preserved, while the surrounding structures were demolished. Others have been made into malls, universities, and other structures. The Northern Michigan Asylum, in Traverse City, was reopened in 2005 as the Village, a complex of shops, restaurants, and residences. The Hudson River Psychiatric Hospital, in Poughkeepsie, New York, after sustaining damage from a lightning strike and two subsequent fires, is likewise being reborn as a mixed-use commercial site. Also in New York, the Buffalo State Asylum for the Insane is in the process of being transformed into a hotel and conference center.
Other buildings have not fared as well. The city of Morristown solicited redevelopment bids for Greystone, but despite receiving six serious proposals from developers, it finally opted to spend $50 million to tear down the structure. Greystone, like a ghost, did not go quietly. Built with solid concrete, it cost the state more than thirty million dollars to knock it down.
Robert Kirkbride himself is haunted by a different aspect of these asylums: the very materials in their construction. The Northern Michigan Asylum, he points out, is a massive structure built entirely with a form of Michigan pine that has now vanished. Which is to say, these buildings carry another kind of history, another kind of legacy: the raw materials of our changing landscape, an archeology of our past.
The problem of the haunted Kirkbride asylums—behemoth structures that reflect a failed utopian plan, that have lingered long after they fell from vogue—is representative of many civic structures that we’ve come to see as haunted. Victims of changing fortunes, they’ve accrued stories of death, despair, and haunting in part because of their misuse or because the government and the people who built them were attempting to make a statement that no longer resonates in the same way. If the Kirkbride asylums are haunted, they are haunted, you could say, by the difference between how history is conceived and how it plays out.